Publications
When it comes to fighting for health freedom, information is key and knowledge is power. You can find CCHF’s latest content – as well as our archived content – here on our website. From original papers and articles to issues of our quarterly Health Freedom Watch, this is where we add published content to keep you informed.

All
Press Releases
Interviews
Health Freedom Watch
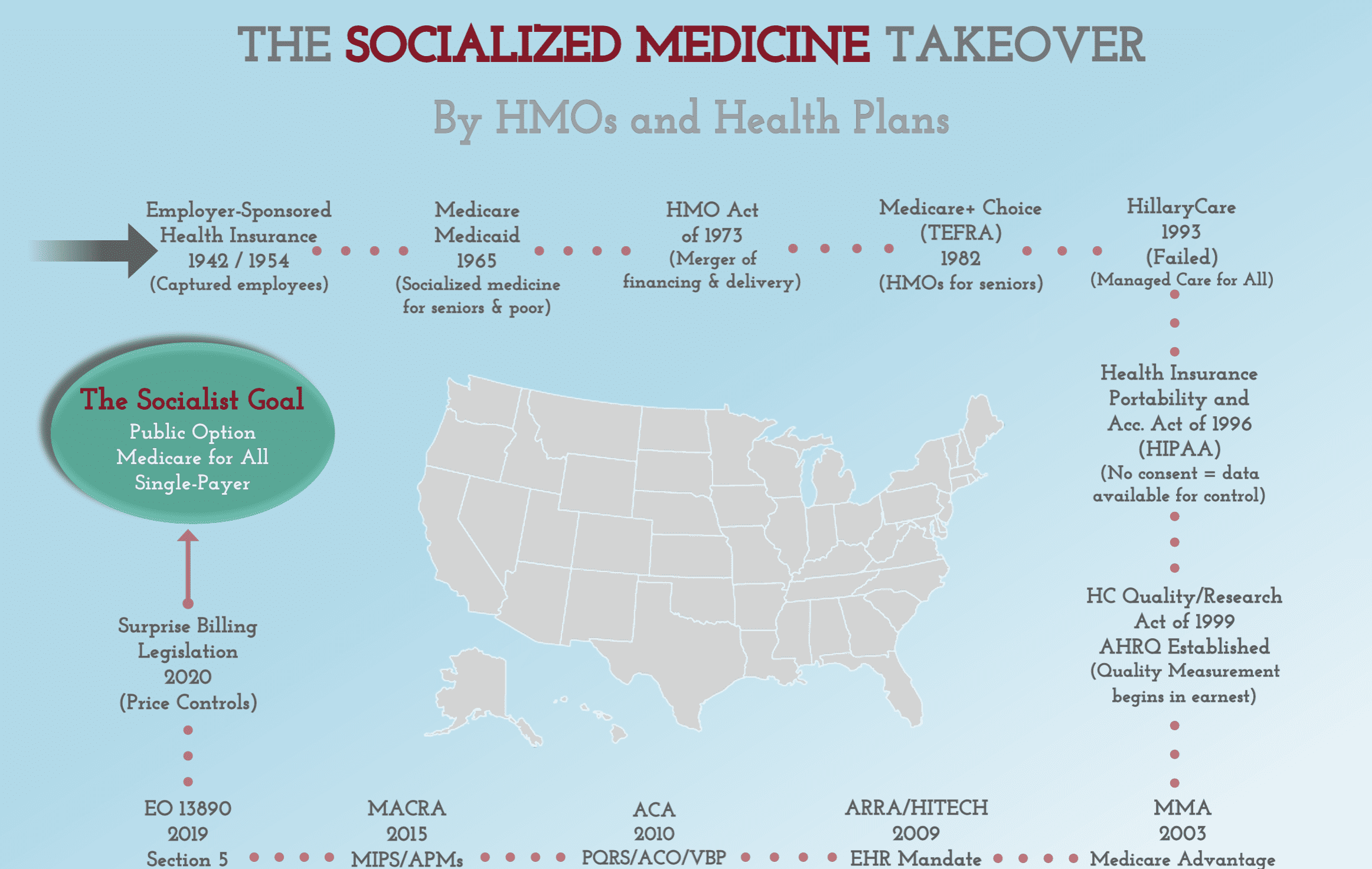
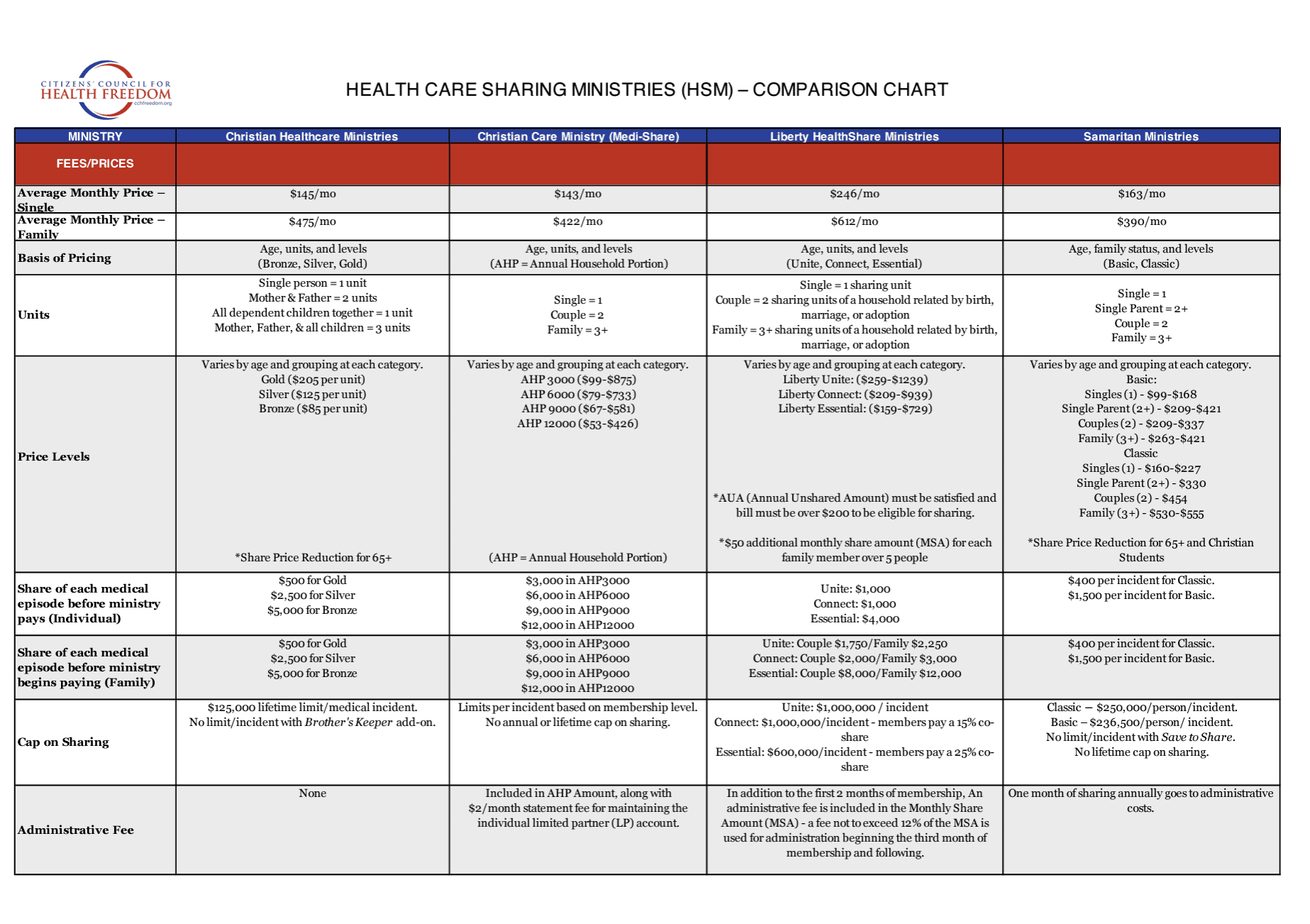
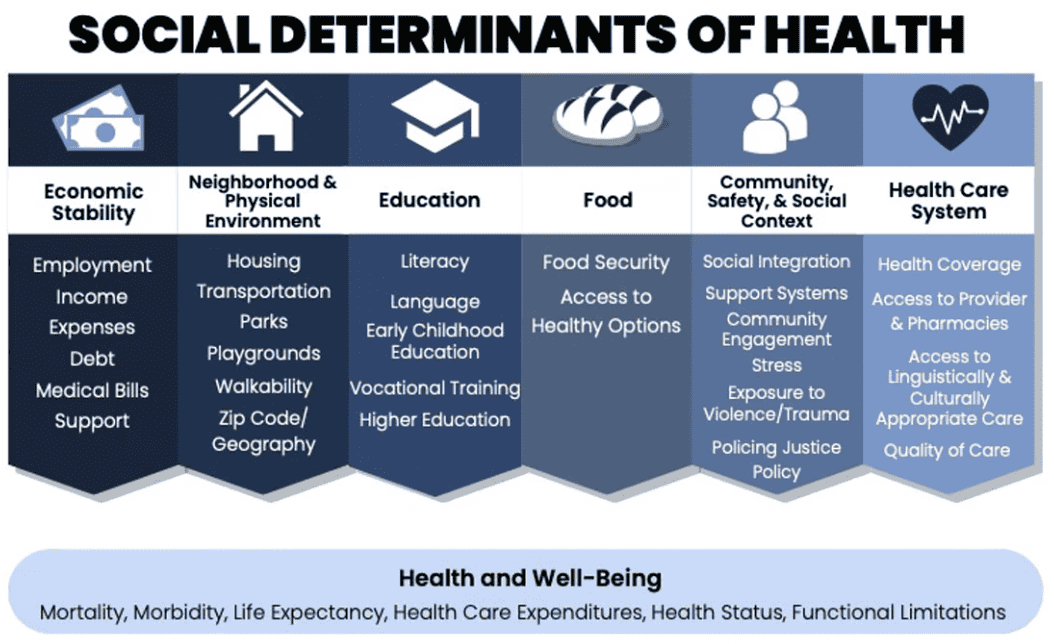
Charts and Diagrams
Testimony and Public Comments
Commentary
National Reports
Health Freedom Handbooks























Load More
Load More
Load More
Load More
Key Initiatives


Subscribe to the Newsletter
Enter your email to begin receiving monthly newsletter emails.
Visited 4,011 times, 336 visit(s) today